 +86-13950196535, 086-592-5566387
+86-13950196535, 086-592-5566387 enquiry@ticarehealth.com
enquiry@ticarehealth.comWe serve all people who pursue high quality and personal customization for healthy life all over the world .
Categories
Latest blog
Airway management is a fundamental aspect of medical care, particularly in emergencies, surgery, and intensive care. Airway management devices are designed to maintain or secure a patient’s airway, ensuring that air can flow freely into the lungs. These devices are critical for patients who are unconscious, unable to breathe adequately, or experiencing respiratory failure. The devices used for airway management are classified into three main categories: non-invasive devices, supraglottic devices, and invasive devices. Each category serves a different clinical purpose and is chosen based on the patient’s condition, the level of support needed, and the clinical setting.
 istock
istock
Non-invasive airway management devices are used to maintain airway patency without entering the trachea. These devices are typically used in patients with partial airway obstruction or when minimal intervention is needed.
Bag-Valve-Mask (BVM) devices are essential for manually assisting ventilation in patients who are not breathing or not breathing adequately. The BVM consists of a self-expanding bag attached to a facial mask, allowing healthcare providers to deliver oxygen or air to the patient’s lungs. The mask fits tightly over the patient’s nose and mouth, creating a seal. Proper technique is required to avoid complications, such as over-inflating the stomach, which can lead to vomiting or aspiration. BVMs are used in emergency situations, during resuscitation, or while awaiting intubation.
The oropharyngeal airway (OPA) is another widely used non-invasive device. It is a rigid, curved plastic tube inserted through the mouth to prevent the tongue from blocking the airway in unconscious patients. OPAs are particularly effective in patients with no gag reflex, such as those in cardiac arrest or during anesthesia. However, they are not suitable for conscious patients because they can trigger a gag reflex and lead to vomiting.
The nasopharyngeal airway (NPA) is a soft, flexible tube that is inserted through the nostrils into the nasopharynx. NPAs are beneficial for patients who have an intact gag reflex, and they are often used in conscious or semi-conscious patients. They provide an effective means to open the airway without triggering discomfort or gagging, making them ideal in cases where the use of an OPA is not appropriate.
 istock
istock
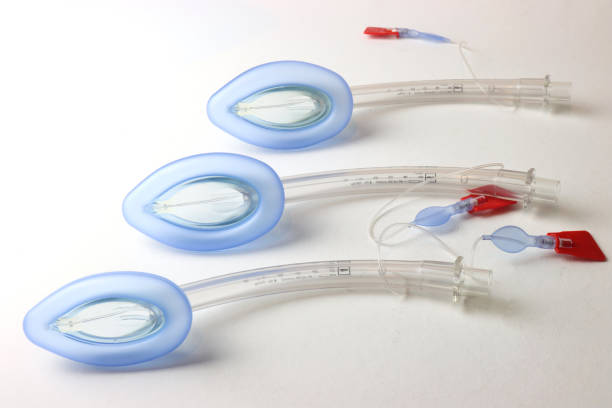
Supraglottic airway devices are designed to sit above the vocal cords and provide an alternative airway in situations where intubation is not immediately necessary. These devices are commonly used for shorter surgical procedures, in emergency situations, or when difficulty in airway management is anticipated.
The laryngeal mask airway (LMA) is one of the most commonly used supraglottic devices. It consists of a mask-like cuff that fits over the larynx and is inflated to form a seal. The LMA provides a secure airway for ventilation and is easier to insert than an endotracheal tube. LMAs are frequently used in anesthesia for routine surgeries and are also used in emergency settings when intubation is challenging. However, LMAs are not suitable for patients who are at risk of aspiration or those requiring long-term airway support.
The I-Gel airway is a newer supraglottic device that has gained popularity for its simplicity and ease of use. Unlike the LMA, the I-Gel does not require inflation to form a seal; instead, it uses a soft, gel-like material that adapts to the patient’s airway. This reduces the risk of over-inflation and tissue damage. The I-Gel is ideal for both routine and emergency airway management and is widely used in pre-hospital care, anesthesia, and resuscitation.
The esophageal-tracheal combitube (ETC) is another supraglottic airway device that is used in emergency situations. This dual-lumen device has two separate tubes—one for the esophagus and the other for the trachea. It is typically inserted blindly and provides ventilation through either the trachea or the esophagus, depending on its placement. The ETC is particularly useful in situations where intubation is difficult, such as in patients with obstructed or collapsed airways.
 istock
istockInvasive airway management devices are used in critical care or emergency settings, where more definitive airway control is required. These devices involve the insertion of tubes directly into the trachea and are essential for long-term ventilation or for patients with significant airway obstruction.
The endotracheal tube (ETT) is the most commonly used invasive device. It is inserted through the mouth or nose into the trachea, usually with the assistance of a laryngoscope, to ensure proper placement. The ETT provides secure ventilation and airway protection by preventing aspiration of gastric contents into the lungs. It is primarily used in surgical procedures, intensive care units, and emergency situations when the patient cannot breathe on their own. However, intubation requires skill and training, and improper placement can lead to complications like trauma to the airway or unintentional esophageal intubation.
For patients who require long-term airway management, a tracheostomy tube is often preferred. This tube is inserted directly into the trachea through a surgical opening in the neck. Tracheostomy tubes offer a more comfortable and sustainable solution for patients who need prolonged mechanical ventilation or those with chronic respiratory conditions. They reduce the risk of airway complications associated with prolonged endotracheal intubation, such as vocal cord damage or tracheal stenosis.
In some emergency situations where other methods of securing the airway are not possible, a cricothyrotomy may be performed. This involves creating an incision through the cricothyroid membrane to establish an airway. A cricothyrotomy is typically performed as a last resort in cases of severe airway obstruction, such as after trauma or when all other airway management options have failed. While life-saving, this procedure requires expertise and carries risks, such as bleeding, infection, or injury to surrounding structures.
Airway management devices are vital tools for healthcare providers to ensure patient safety and effective ventilation in a wide range of clinical settings. From non-invasive options like BVMs and OPAs to more advanced supraglottic and invasive devices, each device is tailored to specific patient needs and clinical scenarios. Understanding the functions, indications, and limitations of these airway devices is essential for healthcare professionals to provide optimal care, whether in emergencies, surgeries, or long-term intensive care settings. Proper training and selection of the right airway device can significantly improve patient outcomes and ensure the secure management of the airway.

sign up for our newsletter to receive the latest news, exclusive offers, and other discount information.







